Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


By the third week, most people are staring into a mirror that has not changed, holding a vial that promised otherwise. The scale is stubborn. The joint still aches on stairs. Somewhere, an ad is still insisting on transformation, and the gap between that promise and the person standing in the bathroom is where a lot of quiet, dangerous decisions get made: doubling a dose, quitting a week too early, believing a forum post over a clinical trial. That gap is the actual subject of this piece, and the only honest fix for it is time, measured the way the science measured it, not the way the marketing does.
Before the specifics: anyone who landed here searching for alternatives to Limitless Life Nootropics, also known as Limitless Biotech, is choosing between one research-chemical vendor and several other paths. The company, founded in 2019 and based in Gulf Breeze, Florida, sells around ninety peptides as vials, capsules, and nasal sprays, every label reading “for research use only” and “not for human consumption.” It runs HPLC and LC-MS testing and posts certificates of analysis without naming the lab doing the work, and its customer reviews split down the middle. That is the plain description, no spin either direction. What follows is the timeline question nobody selling these products wants to answer honestly.
This piece has no affiliation with Limitless Life Nootropics, Limitless Biotech, or any provider named below, and links to none of their storefronts. Every outbound reference points to a primary source anyone can verify: the FDA actions and peer-reviewed trials behind each timeframe here. Compounded and prescribed peptides are not FDA-approved, and products marketed “for research use only” are not approved for human use. Last updated June 2026.
Here is the thread worth pulling on before anything else, because it explains almost everything below. Line up these compounds by how much human trial data backs them, then line them up again by how confidently they’re marketed, and the two lists run in opposite directions. The category with the strongest, longest, most rigorous human trials, GLP-1 weight-loss drugs, is also the one where people are most impatient, expecting in six weeks what the trials took the better part of a year to show. The categories with the thinnest human evidence, recovery peptides and NAD+, are the ones sold with the most specific, most confident timelines. Once that inversion is visible, the rest of this gets easier to read.
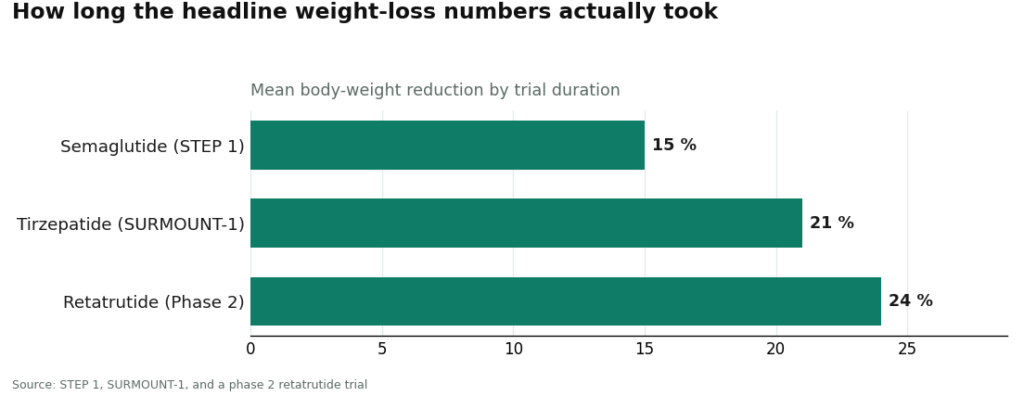
This is the one category here with strong, repeated human data, and the central fact people skip past is that the headline numbers took most of a year to arrive. Not weeks.
The roughly 15 percent mean body-weight reduction attached to semaglutide comes from the STEP 1 trial, which ran 68 weeks [C6]. The roughly 21 percent figure for tirzepatide comes from SURMOUNT-1, run over 72 weeks [C7]. Retatrutide’s roughly 24 percent came out of a phase 2 trial that ran 48 weeks [C8]. Those durations are not a footnote. They are the timeline hiding behind every ad that implies otherwise.
What that means in practice: appetite changes and modest early movement in the first few weeks are real and expected, but the big number is an endpoint reached gradually, over many months, while the dose is deliberately escalated in slow steps. That slow ramp is not caution for its own sake. It’s the mechanism that keeps the treatment tolerable. Pushing the dose faster to speed things along is precisely the self-directed move that unsupervised use invites, and it is where a lot of the harm in this category actually starts.
This is where candor matters most, because it’s also where the marketing gets loudest.
Take BPC-157, a fixture in nearly every catalog including this one. People describe it healing tendons and gut trouble within weeks. What the published science actually shows is overwhelmingly preclinical: a 2026 review lays out its proposed cytoprotective mechanisms across animal injury models [C10]. That’s mechanism and animal data, not large controlled human trials with a schedule anyone could plan around. The honest answer to “how long until this heals my injury” is that there isn’t good human trial evidence that it reliably does, on any timeline.
The practical implication: hold recovery peptides to a different bar than GLP-1s. Don’t build a recovery plan around a timeline the evidence can’t support, and don’t raise the dose because “nothing’s happening by week three.” There is no validated benchmark saying anything should be happening by week three. Thin evidence isn’t proof of nothing, but it does mean anyone using these compounds is running a personal experiment with no map, best done cautiously and ideally with a clinician aware of it, not alone with a thread of anonymous testimonials.
Same candor here, arguably more of it. Longevity peptides, NAD+ and its precursors especially, are sold on a promise that resists any real timeline, because the human evidence doesn’t support a general anti-aging effect to begin with.
What trials do exist are small and tied to specific, rare medical conditions, like a double-blind crossover trial of nicotinamide riboside in patients with Werner syndrome [C11]. That’s a legitimate study, but it says nothing about whether NAD+ injections slow aging in an otherwise healthy person, and there’s no credible timeline for a benefit that hasn’t been demonstrated. When a label promises to make someone “feel younger” by a certain week, that schedule is copywriting, not data.
Worth including one compound where the timeline is both real and modest, because it shows what an honest claim actually looks like.
PT-141, the active molecule in the approved product Vyleesi, has a defined, FDA-recognized use for one specific condition, hypoactive sexual desire disorder in premenopausal women, established across two randomized phase 3 trials [C9]. That’s a genuine, time-bounded effect for a particular situation, and it stays narrow: the approved evidence covers that use, not the wider list of effects the compound gets marketed for elsewhere. A research vial of it isn’t the approved product either. The lesson generalizes: real effects in this category tend to be more specific and more modest than the marketing suggests, and matching expectation to evidence is what keeps someone from being disappointed or hurt.
Here’s a piece of the puzzle the timeline conversation usually skips. Moving to a supervised path doesn’t just reduce risk. It changes how the waiting period is experienced, mostly for the better.
Left alone, the timeline becomes a solo guessing game: watching for effects with no qualified read on whether what’s happening is the compound, the dose, chance, or a problem, and the temptation, when nothing seems to be happening, is to push the dose higher. That’s where a lot of harm begins. A supervised model removes that pressure. A clinician sets a realistic timeline at the start, controls the dose escalation so nobody’s tempted to rush it, and reads the response at defined check-ins, so a stall or a side effect gets managed instead of guessed at. That’s the practical value of a route like FormBlends, which by its own description requires a licensed physician consultation and prescription and dispenses through licensed pharmacies. The timeline becomes something someone qualified is watching, instead of something a person alone has to decide is normal or alarming.
There’s a real cost to that, worth naming honestly. The supervised path is slower up front. There’s an intake, a clinician has to agree, and none of that is as fast as adding a vial to a cart. But that front-loaded friction buys a realistic timeline and a hand on the dose, and over the months that actually matter, that trade tends to be worth far more than the days saved at checkout.
Across all four, supervision changes the texture of the wait: someone qualified is setting expectations, controlling the ramp, and reading the response, instead of leaving a person to guess and, worse, to overdo it out of frustration. That shift toward supervision is accelerating in 2026, the same year regulators put the unsupervised model on notice in writing [C1][C2]. The vials keep promising speed. The evidence keeps promising something real but slower, and being honest about which one is actually being purchased is what keeps a person safe, and keeps them from giving up too early on the part of this that genuinely works.
How long does it realistically take to see meaningful weight loss on a GLP-1 like semaglutide or tirzepatide? Plan on many months, not weeks. The headline numbers came from long trials: roughly 15 percent mean reduction for semaglutide from a 68-week trial [C6], and roughly 21 percent for tirzepatide from a 72-week trial [C7]. Appetite changes and modest early movement can show up in the first few weeks, but the big numbers are an endpoint reached gradually as the dose is escalated slowly on purpose.
Is there a reliable timeline for BPC-157 healing an injury? No. The published evidence is overwhelmingly preclinical, built on animal injury models rather than large controlled human trials [C10]. There’s no validated human schedule saying something “should” be working by a given week, so a confident week-by-week recovery timeline for it is a guess dressed up as fact. Hold it to a different standard than the GLP-1s and resist raising the dose just because nothing seems to be happening.
Do NAD+ or its precursors have a timeline for anti-aging benefits in healthy people? No credible one exists. The human trials that do exist are small and tied to specific medical conditions, like a double-blind crossover trial of nicotinamide riboside in patients with Werner syndrome, a rare disease [C11]. That isn’t evidence that NAD+ slows aging in an otherwise healthy person, so a “feel younger in X weeks” promise is marketing, not data.
Why do clinicians escalate the dose so slowly instead of starting high to get results faster? Because the slow ramp is built into how these medications were studied and is the main lever for tolerability. Chasing quicker results by pushing the dose is exactly the self-directed move the unsupervised model invites, and it’s associated with dosing errors and adverse events in compounded settings [C2]. In a supervised setup, a clinician controls that ramp, which is why the slow start is a feature of the medicine, not caution for its own sake.
Is PT-141 a good example of a peptide with a real, predictable timeline? It’s the honest example, but a narrow one. PT-141, the active molecule in the approved product Vyleesi, has a defined approved use for one condition, hypoactive sexual desire disorder in premenopausal women, established in two randomized phase 3 trials [C9]. That approved evidence covers a single use, taken as needed before activity, not the wider list of effects the compound gets marketed for, and a research vial isn’t the approved product.
Does a supervised provider just make things safer, or does it change the timeline too? Both. A clinician sets a realistic timeline up front, controls the dose escalation so nobody rushes it, and reads the response at check-ins, so a stall or side effect gets addressed rather than guessed at. The trade-off is a slower start, since intake and clinician sign-off take longer than an online checkout, but that early friction buys a managed timeline across the months that actually count.
Limitless Life Nootropics operated as a research-chemical vendor, not a licensed pharmacy, which puts it in a legally gray zone for many of the peptides and compounds it sold. That doesn’t make every product fake, but it does mean quality control, dosing accuracy, and purity testing aren’t held to the standard regulated sources meet. Buyer protection is thin, and regulatory crackdowns have hit similar vendors repeatedly.
It depends on what someone was trying to accomplish. For peptides or compounded hormones, a physician-supervised compounding pharmacy, such as FormBlends, is the more accountable route, since a licensed provider reviews labs and a pharmacist oversees the formulation. For general cognitive support, reputable supplement brands with third-party testing certificates are a safer starting point than research-chemical sites.
It varies with the compound, baseline health, and whether the previous source was even delivering accurate doses. Most people report noticing meaningful differences somewhere between four and twelve weeks. Anyone switching because the old source had inconsistent quality may need a wash-out period first, before any fair judgment is possible.
Avoid jumping to another unregulated research-chemical site just because it carries familiar product names. The two cleaner options are a licensed compounding pharmacy with a valid prescription route, or established supplement retailers that publish independent third-party certificates of analysis for every batch. Verifying those certificates upfront saves a lot of frustration later.
Written by Ines Turner, longform reporter. Last reviewed January 2026.
For informational purposes. Any new treatment should be reviewed by a licensed professional first.